
PCOS & DYSMENORRHEA
DYSMENORRHEA
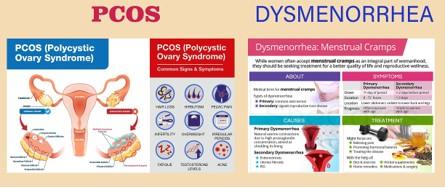
Dysmenorrhea is a medical term that refers to painful menstrual periods. It is a common condition experienced by many women and can range from mild discomfort to severe, debilitating pain
Primary Dysmenorrhea: This type of dysmenorrhea occurs without any underlying medical condition. It usually starts within a few years of starting menstruation (menarche) and is believed to be caused by an excess of prostaglandins, hormone-like substances that cause the uterus to contract during menstruation. Symptoms typically improve with age and may subside after childbirth
Secondary Dysmenorrhea: Secondary dysmenorrhea is associated with an underlying medical condition, such as endometriosis, adenomyosis, pelvic inflammatory disease (PID), fibroids, or ovarian cysts. In these cases, the pain is often more severe and may be accompanied by other symptoms such as heavy menstrual bleeding, irregular periods, or pain during intercourse
Symptoms
PCOS
Polycystic ovary syndrome (PCOS) is a hormonal disorder that affects women of reproductive age. It is characterized by multiple cysts on the ovaries, irregular or absent menstrual periods, and excess levels of male hormones (androgens). PCOS can cause a range of symptoms and has implications for reproductive health, metabolic health, and overall well-being
The exact cause of PCOS is not fully understood, but it is believed to involve a combination of genetic and environmental factors. Insulin resistance, which leads to elevated insulin levels in the blood, is thought to play a central role in the development of PCOS. This can disrupt hormone levels and lead to the characteristic symptoms of the condition
Symptoms
Irregular menstrual periods or no periods at all
Excessive hair growth (hirsutism), particularly on the face, chest, or back
Acne
Weight gain or difficulty losing weight
Thinning hair or hair loss on the scalp (male-pattern baldness)
Darkening of the skin, particularly in skin folds such as the neck creases, groin, or underarms (acanthosis nigricans)
Difficulty getting pregnant (infertility) due to irregular ovulation or lack of ovulation
UTERINE FIBROID
Uterine fibroids, also known as leiomyomas or myomas, are non-cancerous growths that develop in the muscular wall of the uterus. They are the most common type of benign tumor in women of reproductive age and can vary in size, number, and location within the uterus
Causes
The exact cause of uterine fibroids is not fully understood, but they are believed to develop from abnormal growth of smooth muscle cells in the uterine wall. Risk factors for developing fibroids may include hormonal factors (such as estrogen and progesterone), genetics, and other factors such as obesity and age
Symptoms
Many women with uterine fibroids may not experience any symptoms, and the condition is often discovered incidentally during a pelvic exam or imaging test
Heavy menstrual bleeding (menorrhagia): Fibroids can cause prolonged or heavy menstrual periods, sometimes leading to anemia.
Pelvic pain or pressure: Fibroids can cause discomfort or pain in the pelvis, lower back, or abdomen, especially during menstruation or sexual intercourse.
Frequent urination or difficulty emptying the bladder: Large fibroids may press on the bladder, leading to increased urinary frequency or difficulty emptying the bladder completely.
Constipation or difficulty with bowel movements: Fibroids can put pressure on the rectum, leading to constipation or difficulty passing stools.
Enlarged abdomen or visible swelling: Large fibroids may cause the uterus to enlarge, leading to a feeling of fullness or visible abdominal swelling
Diagnosis
Uterine fibroids are typically diagnosed through a combination of medical history, pelvic examination, and imaging tests such as ultrasound, MRI, or hysterosonography (ultrasound with saline infusion)